Perfectionists want to get everything just as they want which is not always possible. Avoidance is ignoring the issue and refusal to face it or accept it.
Procrastination means putting off what we know we need to do, i.e., postponing the things like ‘I will do it later’ just to avoid confrontation due to the fear of failure.
(a) How much nutrition one needs depends on one’s activity level, genetic structure,climate and health history. In fact, there is no one diet, which is ideal for everyone, in all situations.
(b) Stress is supposed to affect diet and weight in many wrays. People, who are under stress or in a negative moods are often seen eating more. They seek ‘comfort foods’ or foods that make them feel better.
(c)Stress may increase consumption of less healthy foods. Such people gain weight and loose stamina to fight stress.
(d)Obesity and weight gain is a problem for a section of the society. A much larger section of the society, which is below the poverty line, suffer from malnutrition.
(e)In the condition of poverty, women are the one who are most malnourished. Studies have shown that in India diets of female children and women are inadequate due to discriminatory practices.
•Exercise is directly related to promoting positive health.
•Two kinds of physical exercises essential for good health are ‘stretching exercises’ such as yogic asanas and ‘aerobic exercises’ such as jogging, swimming and cycling.
•Stretching exercises have a calming effect.
•Aerobic exercises increase the arousal level of the body.
•Yogic asanas provide systematic stretching to all the muscles and joints of the body and massages the glands and other body organs.
•Regular exercise reduces stress because it improves efficiency of vital body organs and improves immune system.
•Positive health and well-being come through a positive attitude of the mind.
•Positive health is the state of complete physical, mental, social and spiritual well¬being. It is not merely the absence of disease.
•Positive health comprises high quality of personal relationships, a sense of purpose in life, self regard, mastery of life skills and resilience to stress, trauma and change.
•Perceiving the reality fairly accurately.
•Tolerating and understanding different points of view.
•Having a sense of purpose in life.
•Having a sense of responsibility, accepting blame for failures and taking credit for success.
•Being open to new ideas, activities, or ways of doing things.
•Having a good sense of humour, to be able to laugh at oneself and absurdities of life helps to see things in their proper perspective.
•Positive thinking leads to a belief that adversity can be handled successfully whereas negative thinking and pessimism anticipate disaster.
•Optimism, which is the inclination to expect favourable life outcomes is directly linked to psychological and physical well-being.
•Optimists use more problem-focused coping and seek advice and help from others. This optimism function helps the individual to cope up stress effectively.
The white blood cells (leucocytes) within the immune system identify and destroy foreign bodies (antigens) such as viruses. It also leads to the production of antibodies. There are several kinds of white blood cells or leucocytes within the immune system, including T cells, B cells and natural killer cells. T cells destroy invaders, and T-helper cells increase immunological activity. It is these T-helper cells that are attacked by the Human Immuno Deficiency Virus (HIV), the virus causing Acquired Immuno Deficiency Syndrome (AIDS). B cells produce antibodies. Natural killer cells are involved in the fight against both viruses and tumours.
•A person’s response to stress largely depends on how the events are appraised or interpreted.
•This was explained by Lazorus in his Cognitive theory of stress.
•According to this theory, stress depends on his primary or secondary appraisal. A new or changing event is positive, negative or neutral.
•A negative event, such as loosing a long-term job, can be appraisal for its harm, instead a challenge.
•If it is appraised as a threat, which may result in future damage, it will result in high levels of stress.
•If it appraised as a challenge, then the individual, who lost the job, will have more confident expectations of the ability to cope with the stressful event, overcome it.
•If appraised as a harm, assessment of the damage, which has already been caused by the event, will result in high stress.
•Through secondary apptaisal, one’s coping abilities and resources are analysed as to whether they are sufficient in meeting the harm, threat or challenge.
1.Obtaining information about a stressful situation.
2.Deciding our priorities.
3.Dealing directly with the stressful situation.
Such an approach helps during exams and project deadlines.
I would also suggest the adoption of positive attitude and thinking which promotes health and well-being.
A positive attitude where the individual has a fairly accurate perception of reality; ability to take credit for success and blame for failure; acceptance and tolerance for other’s view points.
Positive thinking interns of being optimistic. Optimism points towards the inclination to expect favourable life outcomes. An optimist will always use problem-focused coping and try and find the source of stress. Relaxation Techniques, Exercise, Balanced Diet all contribute significantly to stress reduction.
11. Reflect on the environmental factors that have (a)a positive impact on the being and (b) a negative effect.
Ans. Until recently, catastrophic events were not studied systematically, because of their infrequent and unpredictable occurrence. However, because the survivors of these devastating events often experience the severe psychological aftermath termed ‘post-
traumatic stress disorder’.
Whether large-scale natural disasters produce lasting psychological effects, however, remains a source of controversy. Some research shows evidence of long-term psychological effects, whereas other studies show that the psychological impact of natural disasters is minimal.
In certain respects, the psychological trauma that results from human-produced disasters can be more dramatic and long term in its scope than natural disasters. Several factors seem to contribute to this phenomenon. One important factor seems to be control. Human-produced disasters are usually the result of human error; but we expect that adequate precautions will be taken to prevent human error. Thus, when disaster strikes, our expectations are violated, leading to a loss of control. In contrast, we do not expect to have control over hurricanes, earthquakes, or other types of natural disasters and accept them as fate.
A second factor has to do with the consequences associated with each type of disaster.
Natural disasters, while large in scope, tend to be clearly marked and limited in time. In contrast, human-produced disasters—such as the contamination of ground water with toxic chemicals—can, potentially exert their effects for many years. For example, exposure to toxic chemicals can increase people’s risk of developing cancer or produce genetic damage. Moreover, the psychological trauma combined with the uncertainty regarding when or if these consequences will appear can produce chronic stress-related problems.
12. We know that certain life-style factors can cause stress and may lead to diseases like cancer and coronary heart disease, yet we are unable to change our behaviour. Explain 1 why?
Ans. Life-style is the overall pattern of decisions and behaviours that determine a person’s health and quality of life. An individual, when stressed, is more likely to expose himself/herself to pathogens—agents causing physical illness.
Stressed individuals have poor nutritional habits, disturbed sleeping patterns, tendency to engage in health-risking behaviours such as intake of stimulants such as caffeine, alcohol, cigarettes, drugs like tranquil lies such health impairing behaviours develop gradually and provide pleasant experiences temporarily, but have detrimental long-term consequences.
As they are addictive, and pleasurable, individuals using these psychoactive substances are unable to give them up.
•Such type of life-style ultimately cause serious health hazards like cancer, diabetes and coronary heart diseases.
•Knowing that faulty lifystyle causes various physical and psychological hazards.Still people continue, because the consequences and side effects are not likely to occur immediately. Their effects get manifested after several years. So people ignore them. Because they are aware with the side effects. They develop anxiety because of inconsistency in their attitude and behaviour but because this lifestyle becomes a part of their habit pattern. So they find it very difficult to change and continue such hazardous lifestyle and ultimately it causes a stage of burn out.
Class 12 Psychology Chapter 4 Psychological Disorders
NCERT TEXTBOOK QUESTIONS SOLVED
1. Identify the symptoms associated with depression and mania.
Ans. Depression and Mania are mood disorders. These are characterized by disturbances in mood or prolonged maladaptive emotional state.
The main types of mood disorders include:
1. Major Depression disorders 2. Mania 3. Biopolar Disorders
Depression may get manifested as a symptom of a disorder or a major disorder in itself. 1. Major depressive disorders, are defined as a period of depressed mood and/or loss of interest or pleasure in most activities, together with other symptoms which may include.
Symptoms of Depression:
•Loss of energy, great fatigue.
•Change in body weight,
•Constant sleep problems.
•Tiredness.
•Inability to think clearly.
•Agitation
•Greatly slowed behaviour.
•Thoughts of death and suicide.
•Breakup in relationship.
•Negative self-concept.
•No interest in pleasurable activities.
•Other symptoms include excessive quilt or feelings of worthlessness.
Factors Predisposing towards Depression:
•Genetic make-up
Heredity is an Important risk factor for major depression and bipolar disorders.
•Age is also a risk factor. For instance, women are particularly at risk during young adulthood, while for men the risk is highest in early middle age.
•Gender also plays a great role in this differential risk addition. For example, women in comparison to men are more likely to report a depressive disorder.
•Situational factors like negative life event, lack of social support and not able to live up to expectations etc. are few examples.
2. Mania:
Symptoms of mania.
•Increase in activity level.
•Euphoric.
•Excessively talkative
•Easily distracted.
•Impulsive.
•Less than usual amount of sleep.
•Inflated self esteem.
•Excessive involvement in pleasurable activities.
3.Biopolar Disorders:
Mood disorder, in which both mania and depression are alternately present, is sometimes interrupted by periods of normal mood. This is known as bipolar mood disorder. (Bipolar mood disorders were earlier referred to as manicdepressive disorders.)
•It is cyclic in nature.
•In bipolar disorders, depression alternates with periods of mania, and shows behaviour that is quite opposite to depression.
•In the manic state, the individual turns megalomaniac. Person develops grandiose cognitions and doesn’t consider the negative consequences before acting on these grandiose plans.
•Speech is often rapid, as if she has to say as many words as possible in the time allotted.
•The risk of a suicide attempt is highest in ease of bipolar mood disorders.
2. Describe the characteristics of hyperactive children.
Ans. Achenbach has identified two factors in behavioural disorders:
•Externalizing Factors
•Internalizing Factors
These disorders must manifest before the age of 18.
On the basis of these two factors he classified children’s disorders in two categories:
•The externalizing disorders or undercontrolled emotions: Behaviours that are disruptive and often aggressive and aversive to others in the child’s environment.
•The Internalizing disorders or over-controlled emotions: Those conditions where the child experiences depression, anxiety, and discomfort that may not be evident to others.
1.Externalizing Disorders:
(a)Attention-deficit Hyperactivity Disorder (ADHD).
(b) Oppositional Defiant Disorder (ODD).
(c)Conduct Disorder.
(а)Attention-deficit Hyperactivity Disorder (ADHD):
The two main features of ADHD are:
(i) Inattention (ii) Hyperactivity-impulsivity.
Inattention:
•Children who are inattentive find it difficult to sustain mental effort during work or play.
•They have a hard time keeping their minds on any one thing or in following instructions.
Common complaints are that
•The child does not listen, cannot concentrate, does not follow instructions, is disorganized, easily distracted forgetful, does not finish assignments, and is quick to lose interest in boring activities.
•Children who are impulsive, unable to control their immediate reactions or to think before they act.
•They find it difficult to wait or take turns, have difficulty resisting immediate temptations or delaying gratification.
• Minor mishaps such as knocking things are common whereas more serious accidents and injuries can also occur.
•Hyperactivity also takes many forms. Children with ADHD are in constant notion. Sitting still for some time through a lesson is impossible for them.The child may fidget, squirm, climb and run around the room aimlessly.
•Parents and teachers describe them as ‘driven by a motor’, always on the go, and talk a lot.
•Boys are four times more prone for this diagnosis than girls.
(b)Children with Oppositional Defiant Disorder (ODD):
• Age-inappropriate amounts of stubbornness,
•Irritable, • Defiant, disobedient, and
•Behave in a hostile manner.
Unlike ADHD, the rates of ODD in boys and girls are not very different.
(c) Conduct Disorder and Antisocial Behaviour refer to age-inappropriate actions and attitudes that violate family expectation, societal norms, and the personal or property rights of other.
The behaviours typical of conduct disorder include:
•Aggressive actions that cause or threaten harm to people or animals,
•Non-aggressive conduct that causes property damage,
•Major dishonesty,
•Theft and
•Serious rule violations.
Children show many different types of aggressive behaviour, as—1
•Verbal aggression (i.e., name-calling, swearing),
•Physical aggression (i.e., hitting, fighting),
•Hostile aggression (i.e., directed at inflicting injury to others),
•Proactive aggression (i.e., dominating and bullying others without provocation).
2. Internalizing disorders
(a)Separation Anxiety Disorder (SAD) (b) Depression
(a) Separation anxiety disorder is an internalizing disorder unique to children. Its most prominent symptom is—
•Excessive anxiety or even panic experienced by children at being separated from their parents.
•Have difficulty being in a room by themselves, going to school alone, are fearful of entering new situations, and cling to and shadow their parents’ every move.
•To avoid separation, children with SAD may fuss, scream, throw severe tantrums, or make suicidal gestures.
(b)Depression:
•An infant may show sadness by being passive and unresponsive; a preschooler may appear withdrawn and inhibited; a school-age child may be argumentative and combative; and a teenager may express feelings of guilt and hopelessness.
3. What do you understand by substance abuse and dependence?(Outside Delhi 2009, Delhi Board 2014)
Ans. Disorders relating to maladaptive behaviours resulting from regular and consistent use of the substance involved are called substance abuse disorders.
These disorders include problems associated with using and abusing such drugs as alcohol, cocaine and which alter the way people think, feel and behave.There are two sub-groups of substance-use disorders:
(a)Substance Dependence refers to intense craving for the substance to which the person is addicted.
The person shows tolerance, withdrawal symptoms and compulsive drug taking. Tolerance means that the person has to use more and more of a substance to get the same effect.
Withdrawal refers to physical symptoms that occur when a person stops or cuts down on the use of a psychoactive substance, i.e., a substance that has the ability to change an individual’s consciousness, mood and thinking processes.
(b)Substance Abuse refers to recurrent and significant adverse consequences related to the use of substances.
People, who regularly consume drugs, damage their family and social relationships, perform poorly at work, and create physical hazards.
Substance abuse disorders are a joint result of physiological dependence and psychological dependence. Physiological dependence refers to withdrawal symptoms, i.e., the excessive dependence of the body on drugs. Psychological dependence, on the other hand, refers to the strong craving for a drug because of its pleasurable effects.
The three most common forms of substance abuse:
•Alcohol abuse and dependence • Heroin abuse and dependence
•Cocaine abuse and dependence
Alcohol Abuse and Dependence:
•People, who abuse alcohol, drink large amounts regularly and rely on it to help them face difficult situations.
•Eventually, the drinking interferes with their social behaviour and ability to think and work.
•For many people the pattern of alcohol abuse extends to dependence. That is . their bodies build up a tolerance for alcohol and they need to drink even greater amounts to feel its effects.
•They also experience withdrawal responses when they stop drinking. Alcoholism destroys millions of families and careers.
•Intoxicated drivers are responsible for many road accidents.
•It also has serious effects in the children of persons with this disorder.
•These children have higher rates of psychological problems. Particularly anxiety.
•Depression phobias afid substance-related disorders.
•Excessive drinking can seriously damage physical health. Some of the ill effects of alcohol can be been on health and psychological functioning.
Heroin Abuse and Dependence:
•Heroin intake significantly interferes with social and occupational functioning.
•Most abusers further develop a dependence on heroin, revolving their lives around the substance, building up a tolerance for it, and experiencing a withdrawal reaction when they stop taking it.
•The most direct danger of heroin abuse is an overdose, which slows down the respiratory centres in the brain, almost paralyzing breathing, arid in many cases causing death.
•Regular use of cocaine may lead to a pattern of abuse in which the person may be intoxicated throughout the day and function poorly in social relationships and at work.
•It may also cause problem in short-term memory and attention.
•Dependence may develop, so that cocaine dominates the person’s life, more of the drug is needed to get the desired effects and stopping it results in feeling of depression, fatigue, sleep problems, irritability and anxiety.
•Cocaine poses serious dangerous effects on psychological functioning and physical well-being.
4. Can distorted body image lead to eating disorders? Classify the various forms of it.
Ans. Term ‘eating disorder’ refers to serious disruption of the eating habit or the appetite manifested as distorted body image. The main types are:
•Anorexia nervosa
•Bulimia nervosa
•Binge eating
In anorexia nervosa, the individual has:
•A distorted body image that leads him/her to see himself/herself as overweight.
•Often refusing to eat, exercising compulsively and developing unusual habits such as refusing to eat in front of others.
•Anorexic may loose large amounts of weight and even starve himself/herself to death.
In bulimia nervosa,
•The individual may eat excessive amounts of food, then purge his/her body of food by using medicines.such as laxatives or diuretics or by vomiting.
•The person often feels disgusted and ashamed when She/he binges and is relieved of tension and negative emotions after purging.
In binge eating, there are frequent episodes of out-of-control eating.
5. “Physicians make diagnosis looking at a person’s physical symptoms.” How are psychological disorders diagnosed?
Ans. Psychological disorders are diagnosed on the basis of two classifications, i.e., DSM or IV and ICD-X.
•Classification of psychological disorders consists of a list of categories of specific psychological disorders grouped into various classes on the basis of some shared characteristics.
•International Classification of Diseases (ICD-10) is classification of behavioural and mental disorders.
•ICD-10 refers to international classification of diseases and its 10th revision is being used.
•It is developed by WHO under one broad heading ‘Mental Disorders’ which is based on symptoms.
(The classification scheme is officially used in India)
•The American Psychiatric Association (APA) has published an official manual of psychological disorders:
The Diagnostic and Statistical Manual of Mental Disorders, IVth Edition (DSM-IV).
•It Evaluates the patient on five axes or dimensions rather than just one broad aspect of ‘mental disorder’.
•These dimensions relate to biological, psychological, social and other aspects.
Uses of Classification:
•Classifications are useful because they enable psychologists, psychiatrists and social workers to communicate with each other about the disorders.
•Helps in understanding the causes of psychological disorders and the processes involved in their development.
•It helps in Clinical diagnosis.
6. Distinguish between obsessions and compulsions. (Delhi Board 2014)
Ans. • Sometimes anxiety and tension are associated with obsessions—persistent unwanted thoughts, impulses or ideas or compulsions—seemingly irrational behaviours repeatedly carried out in a fixed, repetitive way.
•People with obsessive-compulsive disorders find their obsessions or compulsions distressing and debilitating but feel unable.to stop them,
•The compulsive actions are usually carried on to alleviate the anxiety caused by obsessions.
A person provoked with anxious thoughts may try to block them out by compulsively counting steps while walking. Another person obsessed with the idea that he is guilty or dirty, may wash his hands every few minutes, sometimes till the bleed.
•The symptoms of OCD include a contamination – an obsession of contamination followed by washing or compulsive avoidance of the object. Shame and disgust and the feeling of being easily contaminated are common. Patients usually believe that the contamination is spread from object to object or person to person by the slightest contact.
(a)Pathological Doubt—Obsession of doubt followed by the compulsion of checking. Patients have an obsessional self-doubt and are always feeling guilty about having forgotten something. The checking may involve multiple trips back – to the house to check the stove.
(b)Intrusive Thoughts—repetitive thoughts of a sexual or aggressive act that is reprehensible to the patient. This is usually not followed by compulsions. .
(c)Symmetry—he need for symmetry and precision, which can lead to a compulsion of slowness. Patients can literally take an hour to shave their faces or eat a meal.
(d)Other symptom patterns may include religions obsessions and compulsive hoardings as well as trichotillomania (compulsive half pulling) and nail-biting.
7. Can a long-standing pattern of deviant behaviour be considered abnormal? Elaborate.
Ans. • Abnormal behaviour is a relative term. It is a matter of degree. It is qualitative
difference. There is no quantitative difference between normal and abnormal.
•The word ‘Abnormal’ literally means away from the normal. It implies deviation from some clearly defined norms or standards.
•Various Views to explain Abnormality:
1.Abnormality as Deviation from Social Norms:
•Each society has social norms, which are stated or unstated rules for proper conduct. Behaviours, thoughts and emotions that break societal norms are called abnormal.
•Behaviour violates social norms or threatens or makes anxious those observing it. Violation of norms makes abnormality a relative concept; various forms of unusual behavioural can be tolerated depending on the prevailing cultural norms. Yet this component is also at once too broad and too narrow.
•A society’s values may change over time. Serious questions have been raised about this definition.
•It is based on the assumption that socially accepted behaviour is not abnormal, and that normality is nothing more than conformity to social norms.
•This approach has major shortcomings and there are serious questions against this approach.
2. Abnormality in terms of Maladaptive Behaviour:
•Recent approach views abnormal behaviour as maladaptive. Many psychologists believe that the best criterion for determining the normality of behaviour is not whether society accepts it but whether it facilitates the well-being of the individual and eventually of the group to which he/she belongs.
•Well-being is not simply maintenance and survival but also includes growth and fulfilment. Maladaptive behaviour refers to—Behaviour that causes problems in life.
— It is inadequate reaction to the stressful situation.
— It ranges from relatively minor but troubling fears to severe distortions of reality.
3. Concept of four D’s: Now-a-days many psychologists believe that if an individual’s behaviour manifests significant deviance, distress, danger and dysfunction in his/ her behavioural pattern, then it should be treated as abnormal.
8. While speaking in public, the patient changes topics frequently. Is this a positive or a negative symptom of schizophrenia? Describe the other symptoms and sub-types of schizophrenia.
Ans. While speaking in public, the patient changes topics frequently. This is a symptom of derailment. This is one of the positive symptoms of schizophrenia; is the descriptive term to a group of psychotic disorders in which personal, social and occupational functioning deteriorate as a result of disturbed thought processes, strong perceptions, unusual emotional states, and motor abnormalities. .
The social and psychological causes of schizophrenia are tremendous, both to patients as well as to their families and society.
Symptoms of schizophrenia:
•Positive Symptoms—comprise excesses and provide reduction of distress in the patient. It comprises excesses of thought, emotion, and behaviour.
•Negative Symptoms—deficits of thought, emotion and behaviour.
• Psychomotor Symptoms.
Positive Symptoms of’Pathological Excesses :
1.Disorganized Thinking and Speech:
•People with schizophrenia may not be able to think logically, and may speak in peculiar ways.
•Formal thought disorders can make communication extremely difficult.
•It refers to problems in the organization of ideas and in speaking so that a listener can understand.
•These include derailment, i.e., rapidly shifting from one topic to another so that the normal structure of thinking becomes illogical (loosening of association, derailed)
•Inventing new words, phrases, i.e., neologism and persistent and inappropriate repetition of the same thoughts.
2.Delusion: It is a false belief that is firmly held on inadequate grounds. It is not affected by emotional argument, and has no basis in reality.
•Delusion of Persecution: belief that they are being plotted against, spied on, slandered, threatened, attacked or deliberately victimized.
•Delusions of Reference: in which they attach special and personal meaning to the actions of others or to objects and event. They believe that they can read others mind.
•Delusions of Grandeur: people believe themselves to be specially empowered with supernatural powers.
•Delusions of Control: they believe that their feelings, thoughts and actions are controlled by others.
3. Hallucinations: Perceptions that occur in the absence of external stimuli.
•Auditory hallucinations are most common in schizophrenia. Patients hear sounds or voices that speak words, phrases and sentences directly to the patients (second person hallucination) or talk to one another referring to the patient as he/she (third person hallucination).
•Tactile hallucinations (i.e., forms of tingling, burning).
•Somatic hallucinations (i.e., something happening inside the body such as a snake crawling inside one’s stomach)
•Visual hallucinations (i.e., vague perceptions of colour or distinct visions of people or objects).
•Gustatory hallucinations (i.e., food or drink taste strange).
•Olfactory hallucinations (i.e., smell of smoke).
4. Inappropriate Effect, i.e., emotions that are unsuited to the situation.
Negative symptoms are ‘pathological deficits’
•Alogia—poverty of speech, i.e., a reduction in speech and speech content.
•Blunted effect—reduced expression of emotions.
•Flat effect—no expression of emotions.
•Avolition—social withdrawal.
Psychomotor Symptoms:
•Schizophrenics move less spontaneously or make odd gestures. These symptoms may take extreme forms known as catatonia.
•Catatonic stupor: motionless and silent for long stretches of time.
•Catatonic rigidity: maintaining a rigid, upright posture for hours.
•Catatonic posturing: assuming awkward, bizarre positions for long periods.
9. What do you understand by the term ‘dissociation’? Discuss its various forms.(Delhi Board 2008, 2010)
Ans. • According to Freud, the anxiety and conflicts were believed to be converted into physical symptoms.
•Dissociation can be viewed as severance of the connections between ideas and emotions.
•Dissociation involves amnesia, feelings of unreality, estrangement, depersonalization and sometimes a loss or shift of identity.
•Sudden temporary alterations of consciousness that blot out painful experiences are a defining characteristic of dissociative disorders.
Four conditions are included in this group—Dissociative amnesia, Dissociative
fugue, disseminative identity disorder and depersonalization.
1. Dissociative Amnesia: is characterized by extensive but selective memory loss that has no organic cause (e.g., head injury). Some people cannot remember anything about their past. Others can no longer recall specific events, people, places, or objects, while their memory for other events remains intact.
• This disorder is often associated with an over-whelming stress.
2. Dissociative Fugue:
Symptoms:
•Unexpected travel away from home or workplace.
•The assumption of a new identity.
•Inability to recall the previous identity.
•The fugue usually ends when the person suddenly ‘wakes up’ with no memory of the events that occurred during the fugue.
3. Dissociative identity disorder, often referred to as multiple personality, is the most dramatic of the dissociative disorders.
•It is often associated with traumatic experiences in childhood.
•The person assumes alternate personalities that may or may not be aware of each other.
4. Depersonalization involves a dreamlike state in which the person has a sense of being separated both from self and from reality.
•In depersonalization, there is a change of self-perception.
•The person’s sense of reality is temporarily lost or changed.
•The patient experiences change in his body parts.
10. What are phobias? If someone had an intense fear of snakes, could this simple phobia be a result of faulty learning? Analyse how this phobia could have developed.
Ans. An intense, persistent irrational fear of something that produces conscious avoidance of the feared subject, activity or situation is called a phobia.
•Phobias can vary in degree and how much they interfere with healthy adaptation to the environment. Some otherwise normal and well-adjusted persons also have phobias.
Phobias are mainly of three types :
1. Specific phobias are those directed towards specific objects and situations and can be varied, e.g., acrophobia (fear of heights), pyrophobia (fear of fire), and hydrophobia (fear of water).
2. Social phobia is a fear of social situations, and people with this phobia may avoid a wide range of situations in which they fear they will be exposed to, scrutinized and possibly humiliated by other people.
3.Agoraphobia: is the term used when people developed a fear of entering unfamiliar situations.
Social learning theories work on the principle that our experience be it positive or negative such as phobia of lizards/cockroaches are the result of learning process which start early in life. Small children can play with snakes; they are not aware of the danger involved. For them it is just another play object, as they grow up the fear of these things are instilled by their parents and society which is reinforced and accounts for reactions like phobia.
A psychoanalytical account for the same could involve attribution to some unconscious > or/and repressed experiences. For example, suppose in your childhood you watched a group of roudy boys brutally torturing a cockroach/snake, which eventually died, although you going about the incidence after some days, but it might remain in back of your mind forever, which might explain your phobia to cockroaches which might remind you of the incidence and disturbs you emotionally.
11.Anxiety has been called the “butterflies in the stomach feeling”. At what stage does anxiety become a disorder? Discuss its types. [Delhi Board 2014 OCD]
Ans. Anxiety is usually defined as a diffused, vague, very unpleasant feeling of fear and apprehension without any apparent reason, therefore it has been called ‘butterflies in the stomach’.
Anxious individual shows combinations of the following symptoms:
Rapid heart-rate, Shortness of breath, Diarrhoea, Loss of appetite, Fainting, Dizziness, Sweating, Sleeplessness, Frequent urination, Tremors.
Types of Anxiety Disorder:
There are many types of anxiety disorders:
(а)Generalized anxiety disorder which consists of prolonged, vague, unexplained and intense fears that are not attached to any particular object.
The symptoms include:
•Worry and apprehensive feelings about the future.
•Hyper vigilance, which involves constantly scanning the environment for dangers.
•It is marked by motor tension, as a result of which the person is unable to relax.
•Restlessness.
•Shaky and tense.
Other symptoms of anxiety
(b)Panic disorder—consists of recurrent anxiety attacks in which the person experiences intense terror.
•A panic attack denotes an abrupt attack of intense anxiety, rising to a peak when thoughts of a particular stimuli are present.
•Such thoughts occur in an unpredictable manner.
•It continues for six and seven minutes and then patients becomes normal.
Clinical Features:
•Shortness of breath •Dizziness
•Trembling •Palpitations
•Choking •Nausea
•Chest pain or discomfort •Fear of going crazy
•Losing control or feeling of dying
(c)Phobic Disorders:
•People who have phobias have irrational fears related to specific objects, people, or situations.
•Phobias can be grouped into three main types, i.e., specific phobias, social phobias, and agoraphobia.
•Specific phobias are the most commonly occurring type of phobia. Specific phobias are unwarranted fears caused by the presence or anticipation of a specific object or situation. This group includes irrational fears such as intense fear of a certain type of animal, or insects.
•Social phobias intense and incapacitating fear and embarrassment when dealing with others, e.g., crowded market, fear of closed space and stage fear.
•Agoraphobia: people develop a fear of entering in an unfamiliar situations. Many agoraphobics are afraid of leaving their home. So their ability to carry out normal life activities is severely limited.
(d)Obsessive Compulsive Disorders:
•Obsessive Behaviour: is the inability to stop thinking about a particular idea or topic. The person involved often finds these thoughts to be unpleasant and shameful but can not control them.
•Compulsive Behaviour: Thus is the need to perform certain behaviours over and over again. Many compulsions deal with counting, ordering, checking, touching and washing.
•Obsessive Compulsive Disorder: People affected by this disorder are unable to control their preoccupation with specific ideas and are unable to prevent themselves from repeatedly caring out a particular act or series of acts that affect their ability to carry out normal activities.In OCD unwanted thoughts combine with compulsive acts.
(e)Post-traumatic Stress Disorders:
•People who have been caught in a natural disaster (such as tsunami).
•Victims of bomb blasts by terrorists.
•Serious accident.
•In a war-related situation.
Symptoms:
•Immediate reactions, i.e., denial and disorientation.
•Physiological reactions, e.g., recurrent dreams, nightmares and flashbacks.
•Cognitive reactions, e.g., impaired concentration, memory loss.
•Emotional numbing, e.g., emotional numbness and suicidal tendencies.
•Social reaction, e.g., apathy and withdrawal.
Class 12 Psychology Chapter 5 Therapeutic Approaches And Counselling
1.Describe the nature and scope of psychotherapy. Highlight the importance of therapeutic relationship in psychotherapy. (CBSE 2013, 2014)
Ans. Psychotherapy is a voluntary relationship between two people, one who seeks help and the other who is ready to provide the help, i.e., the therapist. It is given under therapeutic conditions.
Various psychotherapeutic approaches have the following characteristics:
1.All psychotherapies are systematic application of some theory or principle of different therapies.
2.Only trained professionals can practise psychotherapy.
3.Therapeutic situation is a two-way process in which therapist as well as client actively interact.
4.Psychotherapy functions under formation of therapeutic relationship which is confidential, interpersonal and dynamic in nature.
Psychotherapy has very broad scope to deal with disorders which are as follows:
•Reinforcing client’s resolve for betterment.
•Lessening emotional pressure.
•Unfolding the potential for positive growth.
•Modifying habits.
•Changing thinking patterns.
•Increasing self-awareness.
•Improved interpersonal relations and communication.
•Facilitating decision-making.
•Becoming aware of ones preferences in life.
•Development of adaptive behaviour.
Therapeutic Relationship:
The special professional relationship between the client and the therapist is known as therapeutic relationship or alliance.
There are two major components of this relationship:
1.The Contractual Nature of the Relationship in which two willing individuals, the client and the therapist, enter into a partnership which aims at helping the client overcome his problems.
2. Limited Duration of the Therapy: This alliance lasts until the client becomes able to deal with his problems and take control of his life.
Through therapeutic relationship the therapist wins the trust of the client. The quality of this relationship/alliance determines early healing in psychotherapy.
2. What are the different types of psychotherapy? On what basis are they classified?
Ans. Following are the main psychotherapies:
•Psychodynamic Therapy
•Behaviour Therapy
•Humanistic Therapy or Existential Therapy Parameters of classification are as follows :
1.What is the cause of the problem?
(a)Psychodynamic therapy-Intrapsychic conflicts (id, ego and super ego) causes problems.
(b) Behaviour therapy-Faulty learning of behaviours and unrealistic cognition , (thinking process) cause problems.
(c) Existential therapy-Ansviev about the meaning of one’s life and existence is not available.
2. How did the cause come into existence?
(а)Psychodynamic therapy-Intrapsychic conflicts are caused due to unfulfilled desires of childhood or unresolved fears which cause fixation and repression during psycho-sexual stages of life.
(b)Behaviour therapy-Faulty conditioning patterns, faulty learning through improper rewards, faulty thinking and beliefs.
(c) Existential therapy-Current feelings of loneliness, aimless life or meaningless existence.
3. What is the chief method of treatment?
(a)Psychodynamic therapy-Free association and reporting of dream to make the person confront and resolve the conflict.
(b) Behaviour therapy-To identify faulty conditioning patterns and faulty learning
and to challenge the faulty thinking patterns.
(c)Existential therapy-Providing positive, non-judgmental and accepting therapeutic environment. Therapist acts as a facilitator helping client solve his own problems and arrive at solution through personal growth.
4. What is the nature of the therapeutic relationship?
(a)Psychodynamic therapy-Therapist understands the client and is more capable in interpreting his thoughts and feelings.
(b)Behaviour therapy-Therapist is able to identify faulty behaviour and thought patterns and is capable of finding out correct behaviour and realistic thought patterns.
(c)Existential therapy-Therapist provides warm and emphatic relationship helping the client feel secured to explore the causes of his problems himself and herself.
5. What is the chief benefit to the client?
(a)Psychodynamic therapy-Emotional insight to resolve problems.
(b)Behaviour therapy-Adaptive and healthy behaviour and thought pattern to reduce stress.
(c)Existential therapy-Personal growth by increasing understanding of one’s aspirations, emotions and motives.
6. What is the duration of treatment?
(a)Psychodynamic therapy-Classical psychoanalysis lasts for several years. New version? 10-15 sessions.
(b)Behaviour therapy-Short and completed within few months.
(c)Existential therapy-Short and completed within few months.
3. A therapist asks the client to reveal all his/her thoughts including early childhood experiences. Describe the technique and type of therapy being used.
Ans. Psychoanalysis is a method of treatment of neurotic patients which emphasized the
thoughts and experiences of childhood. It was developed by Dr. Sigmund Freud.
The whole modality of treatment occurs in three phases:
1.Initial Phase: The client becomes making client familial with the routines.
•Establishment of a therapeutic relationship with the analyst,
•Relief with the process of recollecting the superficial materials from the unconscious about the past and present troublesome events.
2.Middle Phase: Transference and interpretation are the means of treating the patient.
•Transference: The client starts identifying positively or negatively to the therapist with other significant people often with father and mother, in his childhood.
•Parent-child relationships are often replayed in this way.
•The therapist may be seen as the punitive father or as negligent mother or vice-versa.
•The therapist maintains a non-judgmental yet permissive attitude towards the client and overcomes the resistance showed by the client.
•This whole process is known as transference and when the therapist becomes a substitute for the client in the present is known as transference neurosis.
Stage of Transference Neurosis:
In the process of transference the client acts out his/her frustrations, anger, fear and depression that he/she carried toward that person in the past, but could not express at that time.
• The therapist becomes a substitute for that person in the present.
This substitution which is known as transference neurosis is helpful in making
the therapist aware of the nature of intrapsychic conflicts suffered by the client.
The transference neurosis may develop in two forms:
(i) Positive Transference: Here the client may fall in love with the therapist and seeks the therapist’s approval.
(ii) Negative Transference: When the client develops feeling of hostility, anger and resentment towards the therapist.
•Stage of Resistance: During the process of transference an individual may develop resistance. Since process of transference exposes the unconscious wishes and conflicts, client’s distress level increases and so the client resists transference.
(i) Conscious Resistance: It is present when the client intentionally hides some information.
(ii) Unconscious Resistance: It is present when the client becomes silent during the therapy session or starts coming late for the sessions, flight into sickness or show unwillingness-to talk about certain things, sudden blocks forgetting and so on.
•According to Freud, resistance is patient’s unconscious struggle to prevent painful material from being brought to the surface and faced directly.
•Interpretation: Interpretation is the fundamental mechanism to bring change in the client. Interpretation is done through two analytical techniques:
(i)Confrontation: The therapist points out to the client an aspect of his psyche that must be faced by the client. It is a subtle process and considered to be the pinnacle of psychoanalysis. .
(ii) Clarification: It is the process by which the therapist brings a vague or confusing event into clarity.
Both the process are done by sharpening and pruning of the material which is brought from unconscious to conscious level.
•The therapist highlights certain important aspects and deletes the unimportant ones.
Working Through: The repeated process of using confrontation, clarification and interpretation is known as working through.
•This process helps the patient to understand himself and the source of the problem.
•It integrates the uncovered material into his ego.
•Insight: The end product of working through is insight.
It is a gradual process wherein the unconscious memories are again and again integrated into conscious awareness.
As this process continues, the client starts to understand himself better at an intellectual and emotional level and gains insight into his/her conflicts and problems. The insight is of two types:
(i)Intellectual Insight: It is intellectual understanding of the event.
(ii)Emotional Insight: The emotional understanding, acceptance of one’s irritations due to unpleasant events of the past and the willingness to change emotionally is known as emotional insight.
3. Third Phase:
• Termination: Insight is the end part of therapy. Now the client is supposed to gain new understanding of himself. Conflicts of the past, excessive usage of defence mechanism and physical symptoms are no longer present and he/she becomes a healthy person.
4. Discuss the various techniques used in behaviour therapy. (CBSE 2012)
Ans. The techniques used in behaviour therapy are not based on any unified theory. These are developed on the basis of various principles particularly on classical conditioning, operant conditioning and modelling. The main objective of the techniques are to modify maladaptive behaviour. Negative reinforcement and aversive conditioning are the two major techniques of behaviour modification.
1.Reinforcement Techniques:
(а)Negative Reinforcement: It refers to following an undesired response with an outcome that is painful or not liked. For example, a mother may cover her son’s thumb with a bitter NEEM paste so that he should not develop habit of thumb sucking. Due to the bitterness, the child tries to avoid or withdraw the bitterness of thumb and will leave the habit of thumb-sucking.
Aversive Conditioning:
•It is establishing relationship between undesirable behaviour and aversive consequences.
•Aversive therapy is a therapeutic technique which uses an unpleasant stimulus to change a deviant behaviour.
•It works by pairing together the stimulus that normally invites the deviant behaviour (such as an alcoholic drink or sexual image) with an unpleasant (aversive) stimulus such as an electric shock or a nausea-inducing drug, with repeated presentations.
•The two stimuli become associated and the person develops an aversion toward the stimulus that formerly gave rise to the deviant behaviour.
(b)Positive Reinforcement: If an adaptive behaviour occurs, positive reinforcement may be used by the therapist. For example, the child’s mother may prepare child’s favourite dish on the day when most of the time child was being observed not keeping his thumb in the mouth.
Token Economy: A behaviour therapy is based on positive reinforcement.
•A package or deal is being established between the therapist and the client.
•Persons with behavioural problems can be given a token as a reward every time a wanted behaviour occurs.
•The tokens are collected and exchanged with for a predetermined reward such as outing for the patient or a treat for the child.
•The technique is widely used in hospitals, schools and reformatory.
(c) Differential Reinforcement: In differential reinforcement, both positive and negative reinforcements are used together. By using this method, unwanted behaviour can be reduced and wanted behaviour can be increased simultaneously.
(d) Method of ignoring Unwanted Behaviour: In this method, the therapist positively reinforces the wanted behaviour and ignores the unwanted behaviour. For example, the parents are instructed to praise the child or give chocolate to him or to take him to cinema if the child does not suck the thumb, : but ignore the unwanted behaviour that is sucking the thumb. This method is
less painful and equally effective for modifying the unwanted behaviour.
2. Systematic Desensitisation: It is a technique introduced by Wolpe, for treating phobias or irrational fears. This technique is based on the principle of reciprocal inhibition. This principle states that the presence of two mutually opposing forces forces at the same time, inhibits the weaker force, e.g., distress, at the same time, relaxation, can not occur.
The technique follows four steps:
(i)Initial interview.
(ii)Training in relaxation exercises.
(iii)Preparation of hierarchy of anxiety-provoking situation. This is a subjective process and changes from problem to problem.
(iv) Desensitization: When the client becomes relaxed, he/she is exposed to least anxiety-provoking situation. Over sessions, the client is able to unique more severe fear-provoking situations while maintaining with relaxation. The client gets systematically desensitized to the fear.
3.Modelling: It is the procedure wherein the client learns to behave in a certain way by observing the behaviour of a role model or the therapist.
•It is role playing.
•Vicarious learning (learning by observing others) is used and through a process of rewarding small changes in the behaviour, the client gradually learns to acquire the behaviour of the model.
5.Explain with the help of an example how cognitive distortions take place. (CBSE 2011)
Ans. Aaron Beck devised cognitive therapy.
•It is also known as cognitive restructuring therapy.
•Basic Assumption: Negative thinking, irrational beliefs and faulty generalization caused disorder.
•This therapy believes that repeated cognitive distortions play significant role in causing disorder. Cognitive distortion means way of thinking which are general in nature but which distorts the reality in a negative manner, e.g., persistent negative and irrational thoughts such as: “Nobody loves me”, “I am ugly”, “ I am stupid” etc.
Step I – Analysis of Core Schemata: Childhood experiences provided by the family and society develop core schemata or systems, which include beliefs and action patterns of the individual.
•A client, who was neglected by the parents as a child, develops the core schema of “I am not wanted.” This may be validated by the teachers in the school.
•Such negative automatic thoughts cause cognitive distortions.
•Cognitive distortions are ways of thinking which are general in nature but which distort the reality in a negative manner. Their patterns are called Dysfunctional cognitive structure.
•Repeated occurrence of these distorted thoughts leads to the development of feelings of anxiety and depression.
Treatment Method:
•The therapist uses questioning, which is gentle, non-threatening and non- judgmental, non probing but thought proviking questions.
•The questions make the client to think deeper into her/his assumptions about his life and problems.
•These questions make the client to think in a direction opposite to his negative thoughts and gains insight of his dysfunctional schemas and able to restructure his thoughts in positive direction.
•Beck’s cognitive approach does not attempt to disprove the ideas held by depressed persons, rather the therapist and client work together to identify the individual’s assumptions, beliefs and expectations and to formulate ways of testing them.
Aim of the Therapy:
•Cognitive restructuring by helping people to recognize and reject the false assumptions that are central to their difficulties.
6. Which therapy encourages the client to seek personal growth and actualise their potential? Write about the therapies which are based on this principle. (2009, 2010)
Ans. • The humanistic-existential therapies encourage personal growth and actualize the potential.
Fundamental Assumption:
•The client has the freedom and responsibility to control his/her own behaviour.
•Psychological distress arises from feeling of loneliness, alienation and an inability to find meaning and genuine fulfilment in life.
•All individuals have desire for personal growth and self-actualization and an innate need to grow emotionally.
Causes of Distress:
1.Obstacles created by the society and family to achieve personal growth.
2.Obstacles in attainment of self-actualization, because it requires free emotional expression. ^
Treatment Modalities:
•The therapist is merely facilitator and guide. It is the client who is responsible for the success of the therapy.
•The client initiates the process of self-growth through which healing takes place.
Therapies based on Humanistic-existential Approach:
Logo therapy is a form of existential therapy.
Victor Frankl, a psychiatrist and neurologist propounded logo therapy.
Basic Assumption: ‘Logo’ is the Greek word for ‘soul’ and “logo’ therapy ‘means treatment of the soul’.
•Person’s desire of finding the spiritual truth of ones existence is the source of motivation.
•binding meaning of self even in life-threatening circumstances is process of meaning making.
•There is a spiritual unconscious, which is the store house of love, aesthetic awareness and values of life.
Aim of Therapy: To help the client to find meaning and responsibility in their life irrespective of their life circumstances.
Treatment Modality:
•The therapist emphasizes the unique nature of the patients life and encourages them to find meaning in their life.
•The therapist is open and shares his/her feelings, values and his/her own existence with the client.
•The emphasis is on here and now.
•In the therapy, transference is actively discouraged.
•The goal is to facilitate the client to find meaning of his/her being.
Gestalt Therapy:
•It is humanistic therapy developed by Fritz Pearl and his wife Laima Pearl.
•It helps the client to develop self-awareness and self-acceptance.
•The client is taught to bring his disowned thoughts, conflicts and anxieties to his awareness.
•The therapist does this by encouraging the client to act out or speak out his/her fantasies about feelings and conflicts.
•This therapy can also be used in group setting.
Client-Centered Therapy:
This kind of therapy is developed by Carl Rogers.
•It is based on non-directive approach.
•To understand individual, we must look at the way they experience events rather than at the events themselves.
•The therapy provides a warm relationship in which the client can reconnect with his/her disintegrated feeling.
•The therapist shows empathy, i.e., understanding the client’s experience as if it were his/her own, is warm and has unconditionally positive regard, i.e., total acceptance.
•The therapist reflects the feelings of the clients in a non-judgmental manner. The reflection is achieved by rephrasing the statements of the client, i.e., seeking simple clarifications to enhance the meaning of the clients statements.
•According to this therapy personal relationships improve with an increase in adjustment. In essence, this therapy helps the client to become his/her real self with the therapist working as a facilitator.
7. What are the factors that contribute to healing in psychotherapy? Enumerate some of the alternative therapies. (CBSE 2012)
Ans. There are several factors which contribute to the healing process. Some of these factors are as follows:
•The techniques adopted by the therapist and the implementation of the same with the client.
•The quality of therapeutic alliance—the regular availability of the therapist, and the warmth and empathy provided by the therapist has its importance.
•The quality of emotional unburdening (catharsis) has significant impact on healing.
•Non-specific factors dre associated with psychotherapy. These are patient variable and therapist variable.
•Patient variable refers to attributed to the client, e.g., clients motivation for change and expectation of improvement due to the treatment etc. Therapist variable refers to his/her good mental health, absence of his/her unresolved emotional conflicts and expertise.
Alternative therapies are so called, because they are alternative treatment possibilities to the conventional drug treatment or psychotherapy. There are many alternative therapies such as yoga, meditation, herbal remedies and so on.
1. Yoga is an ancient Indian technique detailed in the Ashtanga Yoga of Patanjali’s Yoga Sutra. Yoga, as it is commonly called today either refers to only the asanas or body positive component or to breathing practices or pranayama or to a combination of the two.
2. Meditation refers to the practice of focusing attention on breath or an object or thought or a mantra.
3. Vipasana Meditation, also known as mindfulness-based meditation, has ,no fixed object or thought to hold the attention. The person possibly observes the various bodily sensation and thoughts that are passing through his awareness.
4. The rapid breathing techniques to induce hyperventilation as in Sudarshana Kriya Yoga (SKY) is found to be a beneficial, low-risk, low-cost, adjunct to the treatment of stress, anxiety, post-traumatic stress disorder (PTSD) depression, stress-related medical illness, substance abuse, and rehabilitations of criminal offenders.
5. Kundalini Yoga taught in USA has found to be effective in treating mental disorders, obsessive-compulsive disorder. It combines pranayama or breathing with chanting of mantras.
8. What are the techniques used in the rehabilitation of the mentally ill?
Ans. Rehabilitation of the mentally ill is necessary to improve their quality of life once their active symptoms are reduced.
•In the case of milder disorders, such as generalized anxiety disorder, reduction of symptoms improves their quality of life and such patients need not to help rehabilitation.
•However in severe mental disorders, such as schizophrenic disorders, reduction of symptoms does not mean that patient is cured. Such patients develop negative symptoms like apathy or lack of motivation and their cognitive social and occupational skills get impaired. So they need rehabilitation.
•Rehabilitation provides:
1.Social Skill Training: It helps the patients to develop interpersonal skills through role play, imitation and instruction.
2.Cognitive Retraining: It helps the patients to improve the basic cognitive
functions of attention, memory and executive functions. ..
3.Occupational Therapy: The patients are taught skills such as candle¬making, paper bag making and weaving to develop work discipline.
4. Vocational Training: When the patient becomes self-sufficient, vocational training is given wherein the patient is helped to gain skills necessary to undertake productive employment.
9. How would a social learning theorist account for a phobic fear of lizards/cockroaches? How yvould a psychoanalyst account for the same phobia? (CBSE 2013)
Ans. Social learning theories work on the principle that our experience—be it positive or negative—such as phobia of lizards/cockroaches are the result of learning process which start early in life. Small children can play with snakes, they sire not aware of the danger involved. For them it is just another play object, as they grow up the fear of these things are instilled by their parents and society which is reinforced and accounts for reactions like phobia.
A psychoanalytical account for the same could involve attribution to some unconscious or/and repressed experiences. For example, suppose in your childhood you watched a group of roudy boys brutally torturing a cockroach/snake, which eventually died, although you going about the incidence after some days, but it might remain in back of your mind forever, which might explain your phobia to cockroaches which might remind you of the incidence and disturbs you emotionally.
10. Should Electro-convulsive Therapy (ECT) be used in the treatment of mental disorders?
Ans. Electro-convulsive Therapy (ECT):
•It is used to alleviate sudden and severe depression.
•In this method one electrode is placed on each side of the person’s temples and a mild current is turned on for a very short period.
•In the beginning, it was done by injecting metrazol and other drugs in mental patients. These shocks are continued until the patient has a seizure, a muscle contraction of the entire body, lasting at least twenty to twenty-five seconds. ECT seems to work at least for some disorders.
•Unfortunately, there are hazardous risk connected with it. There is amnesia for the whole treatment and after several treatments. There is memory impairment, which may last for several weeks. However, no permanent loss of memory occurs. ECT use has declined since 1950.
•ECT is still used in various hospitals in India because it is economical and effective. In my opinion as a last resort this therapy should continue to be used in India.
Drug Therapy:
•It has been used mainly with four types of disorders—schizophrenia, mania, depression and anxiety.
•These drugs are referred as ‘psychotropic drugs’ because their main effect is on psychological behaviour.
•They are also called as ‘antipsychotic drugs’.
•They are used for the treatment of schizophrenia. ‘Antimanic drugs’ are used to treat patients who are highly agitated, excited and at times unmanageable. ‘Antidepressant drugs’ are used for patients having depression and suicidal risk. ‘Antianxiety drugs’ are known to be minor tranquillisers.
11.What kind of problems is cognitive behaviour therapy best suited for?
Ans. CBT is a short and effective treatment for a wide range of psychological disorders such as anxiety, depression, panic attacks and borderline personality, etc.
•It combines cognitive therapy and behavioural technique.
•According to CBT, the cause of client’s distress is biological, psychological and social relations in combination.
•CBT focuses on the biological aspects through relaxation procedures and the psychological ones through behaviour therapy. Social aspects are dealt with environmental manipulations.
•This multi-axial approach makes CBT a comprehensive technique, which is easy to use, applicable to a variety of disorders and has full potential to deal effectively with psychological disorders.
Class 12 Psychology Chapter 6 Attitude And Social Cognition
1.Define attitude. Discuss the components of an attitude.
Ans. Attitudes are state of the mind, set of views or thoughts or ideas regarding some topic which have an evaluative feature (positive, negative or neutral). These are relatively stable predispositions. .
Various components of an attitude are as follows:
(i)The thought component is referred to as the cognitive aspect of attitude.
(ii)The emotional component is known as the affective aspect.
(iii)The tendency to act is called the behavioural (conative) aspect.
These three aspects have been referred to as the A-B-C (affective-behavioural-cognitive)components of attitude. Attitudes are themselves not a tendency to behave or act in certain ways. They are part of cognition, along with an emotional component which cannot be observed from outside.
2.Are attitudes learnt? Explain how?
Ans. By enlarge attitudes are learnt. They are formed on the basis of learning.
Formation of Attitudes: The term ‘attitude formation’ refers to the movement we make from having no attitude toward an object to having a positive or negative attitude. There are some factors which contribute to the formation of attitudes:
1.Learning: The attitudes are acquired through learning. Many of our views are acquired in situations in which we interact with others or merely observe their behaviour.
-Classical Conditioning/Leaming by Association:
•A basic form of learning in which one stimulus, initially neutral, acquires the capacity to evoke reactions through repeated pairing with another stimulus.
•Player often develop a strong liking for the bat by which they made good runs. Many students start liking a subject if they like the teacher.
-Instrumental Conditioning/Leaming Altitude by Reward and Punishment: A basic form of learning in which responses that lead to positive outcomes or that permit avoidance of negative outcomes are strengthened.
•It applies to the situations when people learn attitudes which are systematically rewarded by significant others, such as parents, teachers or friends.
-Observational Learning: A basic form of learning in which individuals acquire new forms of behaviour or through observing others.
•Children are keen observers and learn a whole lot of things from their parents and other family members.
•They learn many attitudes about other ethnic groups, neighbours and idealize simply by observing the behaviours of adults.
2.Learning through Exposure to Information:
•Many attitudes are learnt in a social context without physical presence of others. Print media, electronic media, biographies of self-actualized people facilitate attitude formations.
3.Learning Attitudes through Group or Cultural Norms:
•Norms are unwritten rules of behaviour. Gradually these norms may become part of our social cognition, in the form of attitudes, e.g., offering money, sweets, fruits and flowers in a place of worship is a normative behaviour in various religions. People imitate such behaviour shown by others as socially approved and develop positive attitude towards it.
3.What are the factors that influence the formation of an attitude?
Ans. The following factors provide the context for the learning of attitude through various processes:
(i) Family and School Environment: parents and other family-members play a significant role in attitude formation. Learning of attitudes within the family and school usually takes place by association, through rewards and punishment and through modelling.
(ii)Reference Groups: Attitudes towards political, religious and social groups, occupations, national and other issues are often developed through reference groups. Reference groups indicate to an individual the norms regarding acceptable behaviour and ways of thinking. Various institutions, religion, culture and communities are form of reference groups.
(iii) Personal Experiences: Many attitudes are formed, not in the family environment or through reference groups, but through direct personal experiences which bring about a drastic change in our attitude towards people and our own life.
(iv) Media Related Influences: Technological advances have made audio-visual media and internet as very powerful sources for attitude formation. School textbooks also influence attitude formation. The media can be used to create consumerist attitude. The media can exert both good and bad influences on attitudes.
•Inference: We draw a conclusion about what kind of person the target is.
Some specific qualities, that influence impression formation, are:
•The information presented first has a stronger effect than the information presented at the end. This is called the primacy effect.
•We have a tendency to think that a target person who has one set of positive qualities must also be having other specific positives that are associated with first set. This is known as halo effect, e.g., if we think that a person is ‘tidy’ then we are likely to think that this person must also be hard/working.
•Whatever information comes at the end may have a stronger influence on impression formation. This is known as the recency effect.
9.Explain how the attribution made by an ‘actor’ would be different from that of an ‘observer’.
Ans. Actor observer phenomena refers to the tendency to attribute our own behaviour mainly to situational causes but the behaviour of others mainly to internal (dispositional) cause.
A distinction is found between the attribution that a person makes for actorrole and observer-role.
Person makes attribution for his/her own positive and negative experiences, it is actor role and the attribution made for another person’s positive and negative experience is observer-role.
For example, if we get good marks, we will attribute it to our own ability and hard work (actor-role, internal attribution for a positive experience). If we get bad marks, we will say we were unlucky or test was difficult (actor-role, external attribution for negative experience).
On the other hand, if our classmate gets good marks, we will attribute his/her success to good luck or easy test (observer-role, external attribution for positive experience). If same classmate gets bad marks, we are likely to feel that his/her failure was because of low ability or due to lack of effort (observer-role, internal attribution for a negative experience).
The reason for the difference between the actor and observer roles is that people want to have a nice image of themselves, as compared to others.
10.How does social facilitation take place?
Ans. • It is form of group influence.
•Social facilitation refers to a concept that performance on specific task is influenced by the mere presence of others.
•Norman Triplett observed that individuals show better performance in presence of others, than when they are performing the same task alone.
Better performance in presence of others is because the person experiences arousal, which makes the person react in a more intense manner.
The arousal is because the person feels he or she is being evaluated. Cottrell called this idea evaluation apprehension. The person will be praised if performance is good (reward); is criticised if performance is bad (punishment). We wish to get praise and avoid criticism, therefore we try to perform well and avoid criticism.
As in case of complex task, the person may be afraid of making mistakes. And the fear of criticism or punishment is stronger.
If the others present are also performing same task, this is called a situation of co-action. When task is simple or a familiar one, performance is better under co-action than when the person is alone.
Task performing can be facilitated and improved or inhibited and worsened by the presence of others. If we are working together in a larger group, the less effort each member puts in. This phenomena is called social loafing, based on diffusion of responsibility. Diffusion of responsibility can also be frequently seen in situations where people are expected to help.
11.Explain the concept of pro-social behaviour.
Or
Describe the factors influencing Pro-social behaviour. (CBSE 2013)
Ans. Pro-social behaviour is any positively valued behaviour that does good to another person, is done without any pressure from outside and without any expectation of a reward or a return.
Humans are social beings. Most of their activities are organized with the help of others. We cannot live and grow unless there is support from others. We often engage in helping others. Such efforts are considered as pro-social behaviour. For any behaviour to be pro¬social, it should fulfil the following conditions:
•There has to be an intention to benefit the other person. Any pro-social act, which one accomplishes by compulsion or as a requirement of a job, does not merit to be called ‘pro-social’.
•The behaviour should be considered socially desirable by the other members of the society. Obviously, helping a thief in stealing is not a pro-social behaviour.
•If an act intended to benefit others is also expect to benefit the helper, it cannot be termed as ‘pro-social’.
The intentions and the consequent positive behaviour are more important considerations of pro-social behaviour than the actual benefits.
The other term which are used interchangeably with pro-social behaviour is altruism. The literal meaning of altruism is “doing things or acting for the interest of others without any ulterior motive.” It is a behaviour that reflects an unselfish concern for the welfare of others. All charitable, humanitarian, philanthropic activities, which people do without any self-interest, come under the category of altruism behaviour.
Determinants of Pro-social Behaviour: The pro-social behaviour depends on many factors.
(i)Pro-social behaviour is based on an inborn, natural tendency in human beings to help other members of their own species.
(ii)Pro-social behaviour is influenced by learning through modelling and positive reinforcement in the family.
(iii)Cultural factors influence pro-social behaviour. Some cultures actively encourage people to help the needy and distressed. Individuals in cultures suffering from a shortage of resources may not show a high level of pro-social behaviour.
(iv) Pro-social behaviour is expressed when the situation activates certain ‘social norms’ that require helping others. Three norms have been mentioned in context of pro-social behaviour:
(a)The norms of social responsibility. We should help anyone who needs help without considering any other factors.
(b)The norms of reciprocity. We should help persons who have helped us in the past.
(c)The norms of equity. We should help others whenever we find that it is fair to do so.
(v)Pro-social behaviour is affected by the expected reactions of the person who is being helped. For example, people might be unwilling to give money to a needy person because they feel that the person might feel insulted, or may become dependent.
(vi)Pro-social behaviour is more likely to be shown individuals who have a high level of empathy, that is, the capacity to feel the distress of the person who is to be helped, e.g., Mother Teresa.
Factors inhibiting Pro-social Behaviour:
(a)Diffusion of Responsibility: Pro-social behaviour may be reduced when the number of bystanders is more than one. On the other hand, if there is only one bystander, this person is more likely to take responsibility and actually help the victim. It happens because each person thinks that others will take the responsibility.
(b)Feeling State of the Individual: Person in a bad mood, being busy with one’s own problems or feeling that the person to be helped is responsible for his/her problem, may not help others.
12.Your friend eats too much junk food, how would you be able to bring about a change in his/her attitude towards food?
Ans. Since my friend eats junk food, it will have some reinforcing value to him/her. In order to bring about a change in his/her attitude towards food, following techniques could be used:
First of all what needs to be targeted is ‘the way he/she thinks about junk food, i.e., the cognitive aspect of his/her positive attitude towards junk food. The modification in his/ her attitude can be achieved through using rational as well as emotional appeal and, if required, help of a dietician whose credibility in this area is very high will be of great use. Attitude changes may be brought about by:
1.Encouraging him/her to read about what is required for a healthy development, e.g., minerals etc. which are not found in junk food.
2.Showing him/her the negative consequences of eating junk food like obesity, other health-related problems by exposing him/her to real life examples.
3.Request people around him/her like family-members, elders and teachers whom he/ she likes. If they provide a role model, i.e., not to consume junk food then he/she will imitate their behaviour.
4.Giving his/her choice and space to decide what is right for him/her considering both the aspects of the food and asking him/her to focus and think about the future problems associated with his/her liking.
All these things can bring about cognitive dissonance which might ultimately bring about the attitude change.
Class 12 Psychology Chapter 7 Social Influence And Group Processes
1.Compare and contrast formal and informal groups, and in groups and out groups.
Ans. Formal Groups:
(i)The functions of a formal group are explicitly stated, as in an office organization, or social work club.
(ii)They have rigidly stated functions and the roles of the members are well-defined or imposed.
(iii)Formal groups have a chain of command for decision-making, e.g., military or bureaucracy. .
Informal Groups:
(i)Informal decision-making process may exist as parallel mechanisms.
(ii)Members of informal groups usually feel more comfortable to take decision in informal settings, e.g., tea time group or lunch group.
(iii)There are no elicit rules and regulations for informal group.
In-group:
(i)It is generally considered as ‘me, my, we, or our’ group.
(ii)People in in-group are viewed as having desirable behaviour and admirable traits,
(iii)It is always good, strong, cohesive, kind-hearted, open, relaxing and cool.
Out-group:
(i)It is considered as ‘they’ group.
(ii) Members are often perceived negatively.
(iii) It is always bad, dirty, damaging, dangerous and has people with negative emotions.
2. Are you a member of a certain group? Discuss what motivated are you to join that groups.
Ans. Definitely I am member of various groups. In other words, I will say that there is no dimension of life where I am not related to a group because we all are social beings and for everything, we are dependent on this or that group. There are various reasons which
motivate me and everybody to join a group. Some of them are as follows:
(i)Security: Groups reduce the feeling of insecurity. Being with people gives a sense of comfort and protection.
(ii)Status: When the group is perceived as important high profile and well known, then the members also feel recognized and ‘experience a sense of power’, e.g., being a student of high profile school.
(iii)Self-esteem: Being a member of a prestigious group enhances the individual’s self-concept.
(iv) Satisfaction of one’s Psychological and Social Needs: Groups satisfy one’s social and psychological needs such as sense of belongingness, giving and receiving attention, love and power.
(v)Group Achievement: Groups help in achieving the goals which cannot be attained individually.
(vi)Provide Knowledge and Information: Group membership provides us knowledge and information and broadens our views.
3. How does Tuck man’s stage model help you to understand the formation of groups?
Ans. According to Tuck man, group formation takes place in following stages:
(i)Forming Stage: When group-members first meet, there is a great deal of uncertainty about the group, the goal, and how it is to be achieved.
(ii)Storming: There is a stage of inter group conflict. There is conflict among members about how the target of the group is to be achieved, who is to control the group and its resources, and who is to perform what task.
(iii)Norming: Group-members by this time develop norms related to group behaviour. This leads to development of a positive group identity.
(iv)Performing: At this stage, the structure of the group has evolved and is accepted by group-members. The group moves towards achieving the group goal.
(v)Adjourning Stage: In this stage, once the function is over or goal is achieved, the group may be disbanded.
These stages help in group formation. Which occurs on the basis of following factors:
(i)Proximity: Individuals with similar background, living in the same complex (e.g., going to the same school) may form groups on the basis of proximity.
(ii)Similarity: It has been observed that more the similarity in the attitudes, interest, beliefs and value system of two persons, greater the likelihood that they would form a group.
(iii)Common Motives and Goals: When a number of people have common objectives or goals, they tend to get together and form a group.
4. How do groups influence our behaviour? (CBSE 2008, 2014)
Ans. I.Group influence our behaviour in following three forms:
•‘Social facilitation’ is a form of group influence.
•‘Social facilitation’ refers to a concept that performance on specific task is influenced by the mere presence of others.
•Norman Triplett observed that individuals show better performance in presence of others, than when they are performing the same task alone.
Better performance in presence of others is because the person experiences According to arousal, which makes the person react in a more intense manner.
The arousal is because the person feels he or she is being evaluated. Cottrell called this idea evaluation apprehension. The person will be praised if performance is good (reward), he/she will be criticised if it is bad (punishment). We wish to get praise and avoid criticism, therefore we try to perform well and avoid criticism.
As in case of complex task, the person may be afraid of making mistakes. And the fear of criticism or punishment is stronger.
If the others present are also performing same task, this is called a situation of co action. When task is simple or a familiar one, performance is better under co-action than when the person is alone.
Task performing can be facilitated and improved or inhibited and worsened by the presence of others. If we are working together in a larger group, the less effort each member puts in. This phenomena is called social loafing, based on diffusion of responsibility.
Diffusion of responsibility can also be frequently seen in situations where people are expected to help.
II.‘Social loafing refers to reduction in motivation when people are functioning collectively.
• It is a form of group influence.
(i)Group members feel less responsible for the overall tasks being performed and therefore exert less effort.
(ii)Motivation of members may decrease because they realize that their contributions cannot be evaluated on the individual basis, so to why to work hard.
(iii) The performance of the group is not to be compared with that of the other groups.
(iv)There is improper co-ordination (or no co-ordination) among members.
III.Group polarization is a group influence which refers to the strengthening of groups initial position as a result interaction and discussion.
As a result of group discussion opinion shifts towards more extreme positions than those whicfi they initially held.
In group polarization, it has been found that groups are more likely to take extreme decisions than individuals alone. Group polarization occurs due to the following factors:
(i)In the company of like-minded people, people are likely to hear newer arguments favouring their view-points.
(ii)When people find others also favouring their view-point, they feel that their view is validated by the public. This is a sort of bandwagon effect.
(iii)When people find others having similar views, they are likely to perceive them as in-group.
5.How can you reduce social loafing in groups? Think of any two incidents of social loafing in school. How did you overcome it?
Ans. Social loading is a negative group influence. Which occurs due to defusion of responsibility. For the quality performance of the group, it should be reduced. It can be reduced through the following methods:
(i)By making the efforts of each person identifiable.
(ii)increasing the pressure to work hard (making group-members committed to successful tasks performance).
(iii)increasing the apparent importance or value of a task.
(iv)making people feel that their individual contribution is important.
(v)strengthening group cohesiveness which increases the motivation for successful group outcome.
6.How often do you show conformity in your behaviour? What are the determinants of conformity?
Ans. Conformity: It is a most indirect form of social influence in which individuals change their behaviour or beliefs to correspond more closely to the behaviour of others in the group. It essentially involves yielding to group pressure.
•People conform because it is comfortable.
•Non-conformity is socially undesirable and many a times punishable offence.
•Most people believe that majority is always right, so it is better to conform.
•Whenever individual gets confused and not confident he/she conforms
•Conformity provides assurance that individual is right.
People conform because of two types of influences:
1.Informational Influence, i.e., influence that results from accepting evidence rather than reality.
• It is social influence based on individuals desire to be correct—to possess accurate perceptions of the social world.
We conform because we have a strong desire to hold the right views. We want to be correct about various matters so we turn to other persons for guidance as to what is appropriate, e.g., if children see that, in the colony, no body is playing in the park then they get information from the actions of others that | park should not be used as playground. This is behaving according to evidence
then from reality.
2.Normative influence, i.e., influence based on a person’s desire to be accepted or admired by others. Individual follows the reality and conforms.
We conform in order to meet other’s expectations and so to gain their approval, e.g., if we see rules written on the board outside the park that playing in the park is prohibited then children avoid playing there.
Sheriff’s experiment known as auto-kinetic effect and Asch’s experiment prove that people do get carried away by the social influence whenever taking decisions.
Determinants of Conformity:
The degree of conformity among the group-members is determined by many factors which are as follows:
1.Size of the Group:
(i)Conformity is greater when the group is small. It happens because it is easier for a deviant member to be noticed in a small group.
(ii) In a large group, if there is strong agreement among most of the members, conformity makes the majority and its norms stronger. In such a case, the minority would be more likely to conform because the group pressure would be stronger.
2. Size of the Minority: When the deviating minority size increases, the likelihood , of conformity decreases.
3. Nature of the Task:
•Where there is something like a correct or an incorrect answer, conformity is more.
•Where answers can vary widely without any answer being correct or incorrect,conformity would be less.
4.Public or Private Expression of Behaviour:
•If the group-members are asked to give their answers publicly, conformity is more.
•Less conformity is found under private expression.
5.Personality Characteristics:
•Some individuals have a conforming personality that is tendency to change their behaviour according to what others say or do in most situations and vice- versa.
7. Why do people obey even when they know that their behaviour may be harming others? Explain. (Delhi Board 2014)
Ans. Obedience: It is most direct form of social influence. Obedience refers to accepting commands/orders from the authority. Authority refers to a person who has inherent power to give reward or punishment.
If a person has power over another, obedience can be demanded; such a person usually has the means to enforce orders.
•Milligram’s studies seem to suggest that the ordinary people are willing, may be with some, reluctance, to harm an innocent person if ordered by someone in authority.
It has been observed that obedience to authority relieves the individual from the responsibility of their actions.
•Individual believes that if he/she will not obey then it will attract penalty.
•Authority commands for destructive obedience are gradually increased from lesser to greater levels of violence.
Sometimes events involved in destructive obedience move so quickly, that the people obeying orders have little time for thinking logically.
8.What are the benefits of co-operation?
Ans. Groups may be co-operative or competitive. Technically, the behaviour that yields maximal joint profit for all the parties involved is called co-operation. The behaviour that yields maximal relative gain is labelled competition.
•Co-operative goals are those, which are defined in such a way that each individual can attain the goal if other members are also attaining their goals. There is interdependence in goal attainment.
Effects of co-operation:
•Goal achievement becomes easy.
•Interpersonal relations get strengthened.
•Cohesiveness rises in the group.
•Group-members become ready to work for others.
•Willingness to accept other’s divergent view-point.
9. How is one’s identify formed?
Ans. • Identity refers to the aspect of one’s self-concept that is based on group-membership.
•Our identity tells us what we are in a larger context.
•After one develops an identity, he/she internalises the norms emphasized in a group and adopts them.
•Identity provides a member of a group with a shared set of values, beliefs and goals about the social world.
•Identity helps to co-ordinate attitude and behaviour.
•The development of identity leads to the devaluation of the out group.
10.What are some of the causes of intergroup conflict? Think of any international conflict.
Reflect on the human price of this conflict.
Ans. • Conflict is a process in which either an individual or a group perceives that the others have opposite interest, and both try to contradict each other.
• In such conflicts intense feeling of ‘We’ and ‘They’ dominate.
• Both the groups believe that only their group (in group) will protect their interest.Individual group conflict occurs when the individuals, needs are different from the group’s needs, goals or norms. Inter group conflict refers to the situation of conflict between groups. It often occurs to maintain the identity of the group different and stronger than the other groups.
Some Major Reasons for Group Conflicts:
1.One major reason is lack of communication and faulty communication between both parties. This kind of communication leads to suspicion, i.e., there is a lack of trust, and hence, conflict results.
2. Another reason for inter group conflict is relative deprivation. It arises when members of a group compare themselves with the members of another group, and L perceive that they do not have what they desire to have, which the other group has.
In other words, they feel that they are not doing well in comparison to other groups. This may lead to feelings of deprivation and discontentment, which may trigger conflict.
3. Another cause of conflict arises when one party believes that it is better than the other, and what it is saying should be done. When this does not happen, both parties start accusing each other.
4.A feeling that the other group does not respect the norms of my group, and actually violates those norms, can cause conflict
5.Desire for retaliation for some harm done in the past could be another reason for conflict.
6.Biased perceptions are at the root of most conflicts.
7. Research has shown that when acting in groups, people are more competitive as well as more aggressive than when they are on their own. Groups compete over scarce resource, both material resources (e.g., territory) and money as well as social resources (e.g., respect and esteem).
8.Perceived inequality is another reason for conflict.
9.According to Gardener Murphy most conflicts begin in the minds of men and then go to the field.
Gardener Murphy, in his book ‘In the Minds of Men’, explains intergroup conflicts at three levels:
(a) Structural Level: It includes high rates of poverty, economic and sound stratification, inequality, limited political and social opportunity, e.g., Tribal areas of Jharkhand and West Bengal becoming fertile ground for Naxal movement.
(b) Group Level: Social identity, realistic conflict between groups over resources and unequal power relations between groups lead to conflicts, e.g., Dalits in India or Women Empowerment Movement.
(c) Individual Level: It includes beliefs, biased attitudes and personality characteristics. These are important determinants.
4. Is behaviour always a reflection of one’s attitude? Explain with a relevant example.
Ans. An individual’s attitude may not always be exhibited through behaviour. Likewise one’s actual behaviour may be contrary to one’s attitude towards a particular topic. Psychologists have found that there would be consistency between attitude and behaviour when:
(i)The attitude is strong and occupies a central place in the attitude system.
(ii)The person is aware of his/her attitudes.
(iii)Person’s behaviour is not being watched or evaluated by others.
(iv)Person thinks that the behaviour would have a positive consequences.
Richard La Piere, an American social psychologist, conducted the following study. He asked a Chinese couple to travel across the United States, and stay in different hotels. Only once during these occasions they were refused service by one of the hotels. La Piere sent out questionnaires to managers of hotels and tourist homes in the same areas where the Chinese couple had travelled asking them if they would give accommodation to Chinese guest. A very large percentage said that they would not do so. This response showed a negative attitude towards the Chinese, which was inconsistent with the positive behaviour that was actually shown towards the travelling Chinese couple. Attitudes may not always predict actual pattern of one’s behaviour.
5.Highlight the importance of schemas in social cognition.
Ans.•Social schemas (schemata) are mental structure.
•They function as a framework to process social information. These schemas lead to emergence of prototypes.
•Prototypes are concepts which have most of the defining features of a concept, class or family.
•These are best representatives of the population.
•Various stereotypes emerge from these schemas. In other words stereotypes are category-based schemas.
6. Differentiate between prejudice and stereotype.
Ans. Prejudices are negative attitude.
•These are bias about others.
•Prejudices are baseless and false.
•It refers to biased attitude formed about an individual or a group of people.
•These are usually negative.
•It has three components, i.e., A-B-C-
(a) Affective (Emotional i.e dislike or hatred).
(b)Behavioural (i.e., discrimination).
(c)Cognitive (Believes, i.e., stereotypes).
Stereotypes are cognitive component of prejudice. It is strongly influenced by the processing of incoming social information.
•These are over-generalized beliefs, e.g., girls are talkative.
•Stereotypes are category based schemas.
•These may be positive or negative or neutral.
•Stereotype has no emotional blending.
•From stereotypes, prejudices may emerge very easily.
•Stereotypes are usually formed for the groups.
•Stereotypes are pre conceived notions.
7. Prejudice can exist without discrimination and vice-versa. Comment.
Ans. Prejudices can exist without being shown in the form of discrimination. Similarly,
discrimination can be shown without prejudice.
•Wherever prejudice and discrimination exist, conflicts are very likely to arise between groups within the same society.
•We all witnessed many instances of discrimination, with and without prejudice, based on gender, religion, community, caste, physical handicap, and illnesses such as AIDS.
•Moreover, in many cases, discriminatory behaviour can be curbed by law. But, the cognitive and emotional components of prejudice are more difficult to change.
8. Describe the important factors that influence impression formation.
Ans. Impression formation is a process by which impression about others is converting into more or less induring cognitions or thoughts about them.In short, impression formation is a process through which we draw quick conclusion/ inferences regarding others.
Factors facilitating Impression Formation:
•Nature of the phenomena (familiar or unfamiliar).
•Personality traits of the perceiver.
•Social schemas stored in the mind of perceiver.
•Situational factors.
The process of impression formation consists of the following three sub-processes:
•Selection: We take into account only some bits of information about the target person.
•Organization: the selected information is combined in a systematic way.
Class 12 Psychology Chapter 8 Psychology And Life
1. What do you understand by the term ‘environment’? Explain the different perspectives to understand the human-environment relationship.
Ans. Word ‘environment’ refers to all that is around us. Literally, it means everything that surrounds us including the physical, Social world and cultural environment. In general, it includes all the forces outside the human beings to which they respond in some way. A psycnologist named Stokols proposed three approaches to describe human-environment relationship:
(i)The Minimalist Perspective: This view assumes that physical environment has negligible influence on human behaviour. Both run parallel to each other.
(ii)The Instrumental Perspective: According to this approach, environment is simply provider. It is for the comfort of us. Human beings can use the environment as per their needs.
(iii)The Spiritual Perspective: It refers to the view of the environment as something to be respected and valued rather than exploited. Physical environment and human relationship are interdependent. The traditional Indian view about the environment supports spiritual perspective, worshipping Pipal, respect for rivers and mountains. Chipko Aandolan and movement by Bisnoi Community are examples of Indian perspective.
2.“Human beings affect and are affected by the environment.” Explain this statement with the help of example.
Ans. Environment significantly influences various physical and psychological aspects of human behaviour. Some are as follows:
(a)Environmental Influence on Perception: According to researches, our perception is influenced by the environment in which we live. For example. Tribal societies of Africa living in Circular huts show less error in a geometric illusion (the Muller Lyer illusion) than people from cities, living in houses with angular walls.
(b)Environmental Influence on Emotions: For example, watching quietly flowing river, a smiling flowers or a tranquil mountain top provides joy and happiness.
•Natural disasters, landslides can provide deep depression and sorrow, lack of control over their lives.
•Such an influence is traumatic, changes people’s lives forever, and can last for a long time after the actual event in the form of post-traumatic stress disorder.
(c)Ecological Influence on Occupation, Living style and Attitudes:
(i)The natural environment of a particular region determines the people living in that region will develop what type of societies—may be agricultural or may be industrial.
(ii)In turn, the occupation determines the life-style and attitudes of the residents of a particular geographical region.
Human behaviour particularly influencing on the environment in negative manner. Following are the environmental stressors which effect human beings, although many are created by human beings themselves.
1.Pollution:
(a)Air-pollution: Emission of toxic gases due to automobile and industrial emissions cause adverse effect on the health.
-Air-pollution reduces visibility and leads to eye irritation, headache, fatigue, occurrence of cancer of respiratory system.
(b)Noise or sound pollution: Any sound which an individual finds unpleasant in a particular situation is considered noise or sound-pollution. Noise (sound pollution) leads to adverse psychological effects. It may leads to high level of stress, narrowing of attention, decrease in concentration, etc.
(c)Water-pollution: Various problems related to digestive system and gastrointestinal issues occur due to water-pollution.
2. Noise
Any unpleasant, irritating or interfering sound is called as Noise.
– Noise is an environmental stressor which may affect adversely depending on (a) Predictability (b) Controllability (c) Intensity
3.Crowding and Density:
•Crowding is the subjective feeling of crampedness or being too close to each other. It has negative effects on task performance, personality, interpersonal relationship, general physical and mental health.
•Density is an objective geographical term which refers to number of persons living within the available space, or per square meter area.
4.Natural and Man-made Disasters:
Natural disasters are earthquake, volcanic eruption, windstorm, tornado, cyclone, famine etc.
— There are man-made disasters also; like Bhopal gas tragedy and nuclear bomb explosion in Japan, which not only caused extensive damage to property and physical environment but also had long-term effects on the lives of people.
— Man is largely responsible for regarding the quality of environment that surrounds us. Almost everything humans do has small but cumulative effects on the environment in which we live. e.g., driving a car, using a hair spray, use of refrigerator, etc.
3.What is noise? Discuss the effects of noise on human behaviour.
Ans. Noise is defined as an unwanted sound or sounds that create an effective response. Some may not be disturbed by even a loud-speaker sound, on the other hand, some might even find whistle, tinkling of wind as noise. Thus, any sound “which an individual finds unwanted is noise.”
Noise (sound pollution) leads to adverse psychological effects. How the noise affect the individual depends on:
(a)its intensity (loudness), loud sound is often unpleasant and irritating.
(b)predictability, we can adapt more easily to a regular, predictable sound such as ‘ chirping of birds in the morning.
(c)Perceived Control: The negative effects of noise are reduced when individuals perceive that they have control over it.
Effects of noise (sound-pollution) on task performance:
(i)When the task being performed is a simple mental task, such as addition of numbers, noise does not affect overall performance whether it is loud or soft.
(ii)If the task being performed is very interesting, then, too, the presence of noise does not affect performance.
(iii)When the noise comes at intervals and in an unpredictable way, it is experienced as more disturbing than the noise being continuously present.
(iv)Difficult task performance requires full concentration, then intense, unpredictable and uncontrollable noise reduces the level of task performance. ‘
(iv) When switching off the noise is within the control of the person, the numbers of ’ errors in task performance decrease.
4.What are the salient features of crowding? Explain the major psychological consequences of crowding.
Ans.Crowding: It is psychological crampedness. It manifests following features:
(a) Feeling of discomfort because of too many people or things around us the experience of physical restriction and sometimes the lack of privacy.
(b)Crowding is the person’s reaction to the presence of a large number of persons within a particular area or space.
Features of Crowding; Crowding has the following features:
— Crowding gives feeling of discomfort.
— It gives a feeling that individual privacy is being threatened.
— It gives feeling that individual’s personal space is being invaded.
— It gives negative view of a space around the person.
— Crowding develops feelings of loss of control over social interaction.
Crowding is studied by various psychologists in India and abroad.
Crowding is not always experienced in high density setting nor all people experience its
negative effects. For example, Mela has high density but still people enjoy it.
Effects of Crowding and High Density:
(а)Crowding and High density may lead to abnormal behaviour and aggression. e.g., an increase in population has sometimes been found to be accompanied by an increase in violent crime.
(b)Crowding leads to lowered performance on difficult tasks that involve cognitive processes and has adverse effects on memory and the emotional state.
(c)Children growing up in very crowded households show lower academic performance. They also show a weaker tendency to continue working on a task if they are unsuccessful at it, compared to children growing up in non-crowded households. They experience greater conflicts with parents and get less support from their family members.
(d) The nature of social interaction determines the degree to which an individual will react to crowding. For example, in parties, large number of persons may not cause stress rather it may lead to positive emotional reactions.
(e) Individuals differ in the degree to which they show negative effects of crowding and also in the nature of these reactions.
Two kinds of tolerance can be mentioned that may explain these individual differences: (t) Crowding Tolerance (ii) Competition Tolerance
(i) Crowding Tolerance; It refers to the ability of a person to mentally deal with the high density or crowding environment, e.g., crowded residence.
•It is developed because people can use to manage people around them.
•It is modifying ones perception one holds regarding high density/crowded situations.
•Indians in general have more crowding tolerance.
(ii)Competition Tolerance: It is the ability to put up with a situation in which individuals would have to compete with many others for even basic resources including physical space.
Since there is a greater possibility of competition for resources in a crowded setting, the reaction to that setting would be influenced by the extent of tolerance for competition for resources.
(iii)Cultural Characteristics: It may determine the extent to which a particular environment is judged to be subjectively more crowded or less crowded.
. Why is the concept of‘personal space’ important for human beings? Justify your answer with the help of an example.
Ans. The concept of personal space refers to the personal physical distance that we maintain in our social interaction.
It is important for following reasons:
(i)It explains many of the negative effect of crowding as an environment stressor.
(ii)It tells us about social relations. For examples, two people sitting or standing close tighter are seen to be friends.
It gives us idea about how physical space can be modified in order to reduce stress or discomfort in real life situations.
Everyone has desire of personal space. Males generally have a larger personal space than females. Degree of personal space differ from culture to culture.
Personal space can vary between people, between situations and settings and between cultures. Edward Hall, an anthropologist, mentioned four kinds of interpersonal physical distance—intimate distance, personal distance, social distance and public distance.
6.What do you understand by the term ‘disaster’? List the symptoms of post-traumatic stress disorder. How can it be remedied?
Ans. Natural disaster is an environmental hazard. It is known as disaster because—
•it is mostly unpredictable.
•it causes enormous loss of life and property.
In general, the intensity of reaction is affected by the following:
(i)The severity of the disaster, and the loss incurred both in terms of property and life.
(ii)The individual’s general coping ability.
(iii)Other stressful experiences before the disaster. For e.g., people, who have experienced stress before, may find it more difficult to deal with another difficult and stressful situation. But, there are ways to be prepared to minimize their decussating consequence in the form of:
1.Warning: when cyclones or high tides are predicted, fishermen are asked not to venture into the sea.
2.Safety Measure: Unfortunately, in the case of some natural disasters such as earthquakes, even if prediction is possible, the events came too suddenly for people to be mentally prepared. Therefore tips are given beforehand about to do when there is an earthquake.
3.Treatment of Psychological Disorder: This includes self-help approach as well as professional treatment. According to some experts who deal with PTSD,one of the key attitude to be developed in the survivors is that of ‘self-efficacy’
i.e. that the belief that “I can do it” or “I came out of this phase successfully”.
(a)Immediate Reaction: The immediate reaction after a disaster is commonly manifest in the form of disorientation. People take some time to understand the full meaning of what the disaster has done to them. They may deny to themselves that something terrible has happened.
(b)Physical Reaction:
There is bodily exhaustion even without physical activity such as-
•Sleep disturbances.
•Change in eating pattern.
•Increased heart-beat and blood-pressure.
(c)Emotional Reaction:
•Fear
•Grief
•Irritability
•Anger (why should this happen to me)
•Helplessness
•Hopelessness
•Depression
•Numbness (absolute lack of emotion)
•Guilt feelings for having survived while someone else died
•Lack of interest in routine jobs
(d) Cognitive Reaction:
•Worry • Difficulty in concentration
•Reduced span of attention • Confusion
•Loss of memory • Nightmare of the event
(e) Social Reactions:
•Withdrawal from others
•Getting into conflict with others
•Having frequent arguments with even
•Feeling rejected or left out Very often in the midst of severe emotional reaction to stress, some survivors may develop positive outlook on life with empathy.
7.What is pro-environmental behaviour? How can the environment be protected from pollution? Suggest some strategies.
Ans. Pro-environmental behaviour is the friendly and caring attitude of people who help to prevent environmental degradation and conserve natural resources.
For instance, change in life-style and attitude of the people like conserving energy resources, planting trees, reduction in noise (sound-pollution) and air-pollution.
Some Strategies to Protect Environment are:
(i) Reducing air-pollution by keeping vehicle in good condition or changing to non-fuel driven vehicle, stopping the practice of smoking.
(ii) Reducing noise (sound pollution) by ensuring that noise levels are low. e.g., discouraging needless honking on the road, or making rule regarding noisy music at certain hours.
(iii)Planting trees and ensuring their care.
(iv)Reducing the non-biodegradable packing of consumer goods.
(v)Laws related to construction (especially in urban areas) that violate optimal environment design.
(vi)Saying ‘no’ to plastic use in any form, thus reducing toxic wastes that pollute water, air and the soil.
8.How is ‘poverty’ related to ‘discrimination’? Explain the major psychological effects of poverty and deprivation.
Ans. Poverty is the economic deprivation, associated with low income, hunger, low caste and status.
•Illiteracy, poor housing, over-crowding, lack of public amenities, mal-and under-nutrition, and increased susceptibility to diseases are main features.
•Poverty is an actual shortage of resources so it is objectively defined term.
•Deprivation is subjectively defined. It is more a question of perceiving or thinking that one has got less than what one should have got.
•Poverty is not a necessary condition for experiencing deprivation but a poor person may experience deprivation.
•Social disadvantage is a condition because of which some sections of society are not allowed the same privileges as the east society e.g. caste system.
Effects of Poverty and Deprivation:
(i)Low aspirations and low achievements, low motivation, and high need for dependence is the major effect of poverty and deprivation. They believe that events in their lives are controlled by factor outside them, rather within them.
(ii)With respect to social behaviour, the poor and deprived sections exhibit on attitude of resentment towards the rest of society.
(iiii)With regard to personality:
•The poor and deprived low self-esteem, high anxiety, introversion, and live only in the immediate present rather than being future-oriented.
•The poor and deprived live with a sense of hopelessness, powerlessness, feelings of injustice and experience a loss of identity.
(iv)Researches have proved that prolonged deprivation significantly impair the cognitive functioning of the individual.
(v)With regard to mental health, there is an unquestionable relationship between mental disorder and poverty or deprivation.
(vi)The poor are more likely to suffer from specific mental illness compared to the rich, possibly due to constant worries about basic necessities, feeling of insecurity or inability to get medical faculties especially for mental illness
9.Distinguish between ‘instrumental aggression’ and ‘hostile aggression’. Suggest some strategies to reduce aggression and violence.
Ans. • Aggression: According to psychologists, aggression refers to any behaviour by a person that is intended to cause harm to another person or persons to take revenge. For example, aggression It can be demonstrated in actual action or through the use of harsh words or criticism or even hostile feelings against others.
•Violence: Forceful destructive behaviour towards another person or persons to attain some material gain is violence.
Instrumental Aggression:
The act of aggression is meant to obtain a certain goal or get others, possessions forcefully. For example, A bully slaps a new student in school so that he can snatch the new comer’s chocolate. In violence, individual may or may not have the intention to harm others in terms of revenge. It is forceful destructive behaviour, e.g., hitting a person just to loot his money.
Hostile Aggression:
An expression of anger towards the target, with the intention of harming him/her even if the aggressor does not wish to obtain anything from the victim. For example, A criminal may beat up a person in the community for mentioning his name to the police. Aggression can be reduced by creating the appropriate attitude towards the general problem of growing aggression.
(a)Parenting:
•Parents and teacher should be specially careful not to encourage aggression in any form. The use of punishment to bring about discipline also needs to be changed.
(b)Modelling:
•Opportunities to observe and imitate the behaviour of aggressive models should be reduced drastically.
Portraying aggression as heroic behaviour should be particularly avoided because this may set the stage for learning through observation.
(c)Implementing social justice and equality in society:
•It will help in reducing frustration levels and thereby curb aggressive tendencies at least to some extent.
(d)Inculcating positive attitude towards peace at the level of community or society. The father of our nation, Mahatma Gandhi, gave the world a new view to peace that was not simply the absence of aggression. This was non-violence. It should be taught to the younger generation.
10. Discuss the psychological impact of television viewing on human behaviour. How can its adverse consequences be reduced? Explain.
Ans. Television is one of the useful products of technological progress. It has both positive and negative effects. It has effects on cognitive processes and social behaviour.
1.T.V. provides large amount of information in an attractive form and in visual mode, for which it became a powerful medium of instructions.
2.Excellent programmes emphasise positive interpersonal attitudes and provide useful factual information, teaching children how to design and construct certain objects.
3.T.V. watching may have an adverse effect on children’s ability to concentrate on one target. Their creativity and ability to understand each other through social interaction is also significantly impaired.
4.Reduction in habit of reading and writing skills and also their outdoor activities such as playing is also reduced.
5.Watching violence on T.V. has been linked to greater aggressiveness in the viewers. As children are not mature enough to think of consequences, they simply imitate.
•Some studies pointed out that merely watching violence on the television does not make children more aggressive. Other factors need to be present.
•Other research findings show that watching violence may actually reduce the natural aggressive tendency of the viewers: what is ‘bottled up’ gets an outlet, thus cleans the system. This process is called catharsis.
6. Due to T.V. watching, consumerist attitude has developed. Numerous products are advertised and it is very natural for the viewer to get carried away.
Class 12 Psychology Chapter 9 Developing Psychological Skills
1.What competencies are required for becoming an effective psychologist?
Ans. For becoming an effective psychologists, following competences are essential:
(а)General Skills (b) Observational Skills (c) Specific Skills
(a)General Skills:
•General skills are essential for all professional psychologists.
•These skills include personal as well as intellectual skills.
•Once ensuring that a student has these skills subsequent training in his/her area of specializations to him/her intellectual and personal skill are as follows:
Interpersonal Skills: Ability to listen and be empathic. It may be verbal or non-verbal.
•Cognitive:
— Ability to solve problems — Having curiosity and flexibility
•Affective Skills:
— Openness to ideas — Agreeableness — Honesty
•Expressive skills: Ability to communicate in verbal and non-verbal form.
•Reflective Skills:
— Intrapersonal intelligence —Ability to examine own motives,attitude and behaviour.
•Personal skills:
— Personal hygiene — Time management
(b)Observational Skills:
Psychologists should have training in objectives and systematic observation.
•They should have skill to observe various aspects of surrounding including people and varying events.
•Psychologists should engage in observing people and their actions with following precautions:
— Patience. — Optimistic curiosity.
— Respecting clients privacy.
— Awareness of people reactions, emotions and motivation.
— Training good questions which could be answered during observation.
(c)If the psychologist wants to work in a specialized field then professional training in specific skill development is essential.
The main specific skills are as follows:
(a) communication skills (b) Psychological testing skill
(c) Interviewing skill (d) Counselling skill
2.What are the generic skills needed by all psychologists?
Ans. General/Generic Skills:
•These are essential for all professional psychologists.
•These skills include personal as well as intellectual skills.
Generic (intellectual and personal skills) are as follows:
Interpersonal Skills: Ability to listen and be empathic. It may be verbal or non-verbal.
•Cognitive:
— Ability to solve problems — Having curiosity and flexibility
•Affective Skills:
— Openness to ideas — Agreeableness — Honesty
•Expressive Skills: Ability to communicate in verbal and non-verbal form.
•Reflective Skills:
— Intrapersonal intelligence
— Ability to examine own motives, attitude and behaviour.
•Personal skills:
— Personal hygiene — Time management
3.Define communication. Which component of the communication process is most important? Justify your answer with relevant examples.
Ans.Communication is a conscious or unconscious, intentional or unintentional process in which feelings and ideas are expressed as verbal and/or non-verbal messages that are sent, received and comprehended.
Component of the Communication:
The mort important component of communication is speaking with the use of language.
•Language involves use of vocabulary which includes words by symbols.
•Communicator must know how to use words appropriately in organized and understandable form.
•It is necessary to be clear and precise.
•Communication takes place within a context and needs to consider the other’s frame of reference.
•It is important for the speaker to adjust his vocabulary level and choice of words to
fit the level of the listener.
•Slang expressions, words unique to a culture, euphemism can become obstacles in good communication.
•Listening may appear as a passive behaviour, as it involves silence. But this is far from true.
•Listening requires a person to be attentive, patient, non-judgmental and have the capacity to analyze and respond.
•It is an active process.
•Hearing and listening are not the same, hearing is biological mechanism. It involves reception of a message through sensory channels.
4.Describe the set of competencies that must be kept in mind while administering a psychological test.
Ans.•Developing the skills of psychological testing is important since tests are important tools used for the assessment of individuals for various purposes. Proper training is required for administration, scoring and interpretation of tests.
•Psychologists study individuals, differences based on factors such as occupation, age, gender, education, culture, etc.
•While using psychological test, following factors must be kept in mind:
1.An attitude of objectivity 2. Scientific orientation
3. Standardised Interpretation must be kept in mind. For example, in organizational and personnel work, in business and industry, where specialized tests are used to select individuals for specific jobs, it is essential to use actual performance records or ratings as a criterion for establishing validity of a test.
•Suppose the personnel department wants to know whether a certain psychological test can help it to identify potentiality of best stenographers.
•It must be established that the test differentiates among employees of several performance levels.
•It should be found the performance on the job of a newly employed worker selected on the basis of test indeed matches with his/her test scores.
5.What is the typical format of a counselling interview?
Ans. Interview refers to purposeful conversation through face-to-face interactions.
•It follows a basic question-answer format.
•First, the objectives of the interview are set.
•The interviewer then prepares on interview format.
•There is a basic format which is followed, regardless of the interview’s purpose; i.e., an interview has three stages:
— Opening — The body — The closing
A.Opening of the Interview:
1. In involves establishing report between the two communicators, so that the interview becomes comfortable.
2. Generally, the interviewer starts the conversation and does most of the talking at the outset. This serves two functions:
(a)It establishes the goal of the interview
(b)It gives the interviewee time to become comfortable with the situation and the interviewer.
B. Body of the Interview:
1.This is the heart of the process.
2.In this stage, the interviewer asks questions in an attempt to generate information and data that are required to fulfil/required for the purpose.
Sequence of Questions:
To accomplish the purpose of an interview, the interviewer prepares set of questions – called a schedule for different domains or categories he/she wants to cover.
1.To form the schedule, the interviewer must first decide on the domain/categories under which information is to be generated. For example for questions used in job interview (box 9.5), the interviewer selected various categories such as not use’ of the organization last worked for, satisfaction with the past job, views on product etc.
2.These domains/categories and the questions within them are formed ranging from easy to answer to difficult to answer.
C. Closing of the Interview:
While closing the interview, the interviewer should:
1.Summarise what she/he has been able to gather.
2.Give a chance to the interviewee to ask questions or offer comments. One ‘ should end witfc a discussion of the next step to be taken.


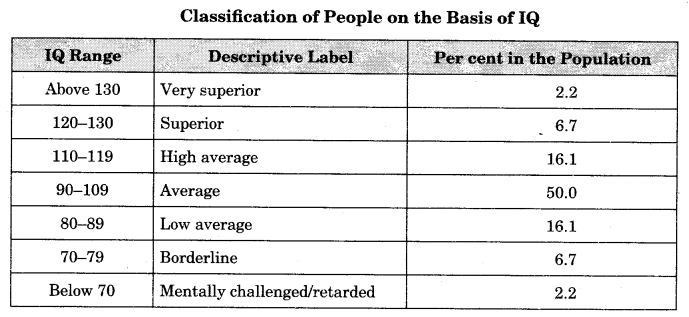
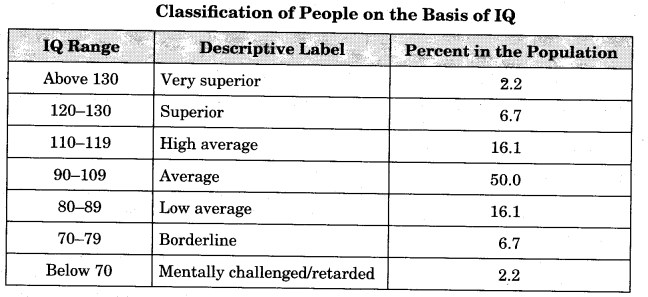






0 Comments